
Diet and Health
Background
Let food be thy medicine and medicine be thy food.
– Hippocrates

Hominy, or nixtamalized maize.
Many traditional food processing techniques increase the availability of nutrients. Early Central American peoples, for example, prepared corn by soaking and cooking it in wood ashes. The process, called nixtamalization, made corn easier to grind and increased the availability of niacin, a B vitamin. When corn was later adopted as a staple crop among Europeans, they neglected to nixtamalize it, resulting in widespread niacin deficiency.
Photo credit: Geoff Lane, 2008. Creative Commons CC BY-SA 3.0.
Early civilizations recognized the profound effects of diet on health. Ancient Central American peoples, for example, prepared corn by soaking it in diluted wood ash and lime (the minerals, not the fruit)—a process that increases the availability of niacin, an essential B vitamin. Early Americans didn’t know about niacin, or at least not as we understand it today, but they somehow learned that preparing corn a certain way was important for their health.1
When corn was later adopted as a staple crop by Europeans, they didn’t know the value of preparing it with ash, and large segments of the population became sick. It wasn’t until the early 1900s that scientists in the U.S. discovered severe niacin deficiency was causing the illness.2
Today, scientists are still learning—and rediscovering traditional knowledge—about how best to eat for health. In industrialized countries like the U.S., dietary choices are made more complicated by the unprecedented variety of products on supermarket shelves, including many that are new to this century. What would traditional dietary wisdom say about corn dogs, frosted corn flakes, or high-fructose corn syrup?
Diet-Related Diseases
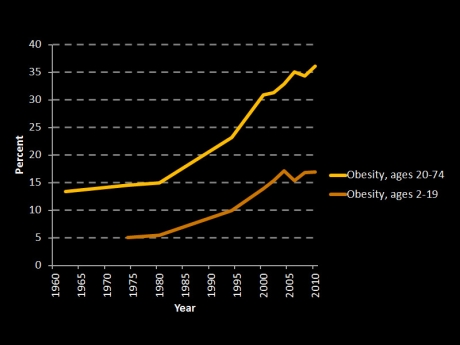
Prevalence of obesity in the U.S., 1962–2010.
One in three American children is overweight or obese, and is predicted to develop type 2 diabetes in their lifetime.5 Because of the rise in obesity, average life expectancy in the U.S. may decline significantly for the first time since the influenza outbreak of 1918.7
Data source: NHANES.9,10
Infectious organisms, such as viruses and parasites, have plagued humanity throughout history. Recent advances in public health, such as vaccines, antibiotics, and improved sanitation, have aided in the fight against infectious diseases—helping people enjoy longer, healthier lives. We now face new challenges, however, in the form of chronic, diet-related diseases:
- Cardiovascular disease is a group of disorders that affect the heart and blood vessels. It is the leading cause of death in the U.S., responsible for an estimated one in three deaths.3
- Cancer is caused by the uncontrolled division of abnormal body cells. It is the second leading cause of death in the U.S. One in five Americans dies from cancer, and four in 10 are expected to receive cancer diagnoses in their lifetimes.4
- Type 2 diabetes is a condition in which cells do not adequately take in glucose (blood sugar) for energy. One in three American children is predicted to develop type 2 diabetes in their lifetime.5
- Overweight and obesity are conditions that usually indicate a high percentage of body fat. Being obese can increase a person’s risk for other diet-related diseases and other health problems such as asthma, sleep apnea (breathing stops and starts during sleep), and pregnancy complications.6 Because obesity rates are so high, life expectancy in the U.S. is predicted to significantly decline for the first time since the influenza outbreak of 1918.7
The causes of these diseases are not fully understood, but scientific evidence gives us clues. Factors such as diet, physical activity levels, genetics, exposure to chemicals in the environment, and even the types of microorganisms living in our guts8 are thought to play a role.
Trends in American Diets
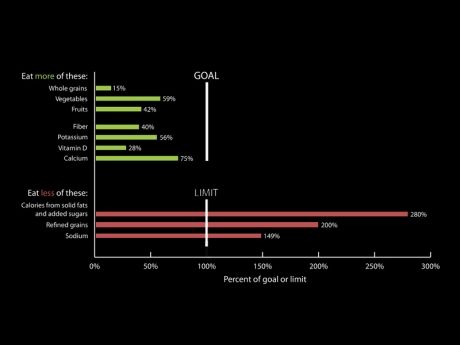
How do typical American diets compare to U.S. dietary guidelines?
Americans' intake of added sugars, refined grains, saturated fats, and sodium greatly exceeds recommended levels, while fruit and vegetable intake falls short. Solid fats (shown on the graph), such as those found in red meat and dairy, contain mostly saturated fat.
Image adapted from: Dietary Guidelines for Americans, 2010.11
The average American consumes more added sugars, refined grains, saturated fats, and sodium than are recommended by U.S. dietary guidelines.11 And while Americans are the second highest per capita consumers of meat in the world,12 their intake of fruits, vegetables, and whole grains remains well below recommended levels. These dietary patterns have been associated with greater risks for diet-related disease.
In many respects, U.S. diets have gotten worse over recent decades. Between 1970 and 2000, the average number of daily calories per capita in the U.S. food supply increased by over 50013—the equivalent of adding a quarter-pound cheeseburger, 365 days a year, to the diet of every U.S. citizen. Much of this growth has been in the form of sugar and refined grains.14
- More added sugar: Between 1970 and 2010, added sugar intake increased by 11 percent.13 While this may not seem like a large increase, added sugar intake was already high in 1970—as much as two 12-ounce cans of soda.
- More soda: Between 1950 and 2000, soft drink consumption more than tripled, while milk consumption nearly halved.15
- More snacks: Between 1977 and 2006, children’s snack consumption doubled.16 By 2006, nearly one-fifth of calories consumed by 2- to 18-year-olds were in the form of grain desserts, pizza, and soda.17
- More high-fat dairy: Between 1970 and 2010, fat intake increased by 73 percent. Much of this was from cheese consumption, which nearly tripled over this same period.13
- More fruits and vegetables (but still not enough): There is some good news. Between 1970 and 2010, vegetable intake increased by 12 percent, and fresh fruit intake increased by 28 percent.13
Eating For Health
Eat food. Not too much. Mostly plants.
– Michael Pollan26

Plant-based foods contain compounds called phytonutrients, many of which have been linked to health benefits. Carotenoids, for example, are plant-based pigments responsible for the orange and red colors of carrots, yams, and tomatoes. Green leafy vegetables also contain carotenoids, but green pigment of chlorophyll masks the orange/red color. Carotenoids are thought to promote heart, eye, and immune system health, and may have cancer-fighting properties.37
Photo credit: USDA. Public domain.
What makes for a healthy diet? Nutritionists generally recommend limiting intake of unhealthy fats, added sugars, red and processed meats, refined grains, and sodium. Here are some of the reasons:
- Diets high in beef, pork, and processed meats (e.g., hot dogs, bacon, and deli meats) have been strongly associated with higher risks of cardiovascular disease,18–21 certain cancers,18,22,23 type 2 diabetes,21,24 and earlier death.18,25
- Diets high in sugar, particularly in sweetened beverages like soda and juice, have been associated with higher risks of obesity,27 type 2 diabetes,24,28,29 and cardiovascular disease.30
- Diets higher in saturated fats (e.g., in red meat and dairy products), and particularly trans fats (e.g., in some snack foods), have been associated with higher risks of cardiovascular disease31–33 and type 2 diabetes.34,35
Eating for health also means enjoying an abundance of health-promoting foods. Fruits, vegetables, and legumes, in particular, are nutrient-dense—they provide a generous amount of vitamins, minerals, and fiber relative to the amount of calories. Nutrient-dense foods tend to take up more space in the stomach, sending signals to the brain that tell us we’ve eaten enough—in contrast to chips, cookies, soda, and other nutrient-poor items that provide a large amount of calories but little or no nutritional value, and encourage overeating because they are not very filling. Healthy fats, found in foods like nuts and avocados, also play important health-promoting roles.
Plant-based foods also contain compounds called phytonutrients. Studies of certain phytonutrients suggest they may offer numerous health benefits, including improved eye, bone, heart, and brain health; immune system support; improved athletic performance; and lower risks of certain diet-related diseases. There are over 20,000 known phytonutrients in edible plants,36 and scientists have only begun to explore their potential.37
Resources
The following list of suggested resources is intended as a starting point for further exploration, and is not in any way comprehensive. Some materials may not reflect the views of the Johns Hopkins Center for a Livable Future.
For teachers
- Why We Eat What We Eat (lesson plan). FoodSpan. Johns Hopkins Center for a Livable Future.
- Introduction to the US Food System: Public Health, Environment, and Equity (textbook). Neff RN (editor). Johns Hopkins Center for a Livable Future. 2014.
Academic journal articles
- Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis (open access). Koeth RA, Wang Z, et al. Nature Medicine. 2013.
- Red meat consumption and mortality: results from 2 prospective cohort studies (open access). Pan A, Sun Q, et al. Archives of Internal Medicine. 2012.
- Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes: A systematic review and meta-analysis (open access). Micha R, Wallace SK, Mozaffarian D. Circulation. 2010.
- Effects on Coronary Heart Disease of Increasing Polyunsaturated Fat in Place of Saturated Fat: A Systematic Review and Meta-Analysis of Randomized Controlled Trials (open access). Mozaffarian D, Micha R, Wallace S. PLOS One. 2010,
- Meat intake and mortality: a prospective study of over half a million people (open access). Sinha R, Cross AJ, et al. Archives of Internal Medicine. 2009.
- Intake of sugar-sweetened beverages and weight gain: a systematic review (open access). Malik VS, Schulze MB, Hu FB. American Journal of Clinical Nutrition. 2006.
- A Potential Decline in Life Expectancy in the United States in the 21st Century (open access). Olshansky SJ, Passaro DJ, et al. New England Journal of Medicine. 2005.
Websites
- Fats and Cholesterol. Harvard School of Public Health.
- Nutrition Action. Center for Science in the Public Interest.
References
- Coe SD. America’s First Cuisines. Austin, TX: Texas University Press; 1994.
- Food and Famine in the 21st Century, Volume 1. William A. Dando (editor). 2012.
- Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6-e245.
- The President’s Cancer Panel. Reducing Environmental Cancer Risk: What We Can Do Now. Washington D.C.; 2010.
- NIH. Healthy weight, healty child. NIH Medlin Plus. 2010;5(2).
- Pi-Sunyer FX. The obesity epidemic: pathophysiology and consequences of obesity. Obes Res. 2002;10 Suppl 2:97S - 104S.
- Olshansky SJ, Passaro DJ, Hershow RC, et al. A potential decline in life expectancy in the United States in the 21st century. N Engl J Med. 2005;352(11):1138-1145.
- Ridaura VK, Faith JJ, Rey FE, et al. Gut microbiota from twins discordant for obesity modulate metabolism in mice. Science. 2013;341(6150):1241214.
- Fryar CD, Carroll MD, Ogden CL. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults: United States, Trends 1960–1962 Through 2009–2010. NCHS Heal E-Stat. 2012.
- Fryar CD, Carroll MD, Ogden CL. Prevalence of Obesity Among Children and Adolescents: United States, Trends 1963-1965 Through 2009-2010. NCHS Heal E-Stat. 2012.
- U.S. Department of Health and Human Services, U.S. Department of Agriculture. Dietary Guidelines for Americans, 2010. 2011.
- FAO. The State of Food and Agriculture: Livestock in the Balance. Rome; 2009.
- USDA Economic Research Service. Loss-Adjusted Food Availability. 2014. http://www.ers.usda.gov/Data/FoodConsumption/FoodGuideSpreadsheets.htm.
- Grotto D, Zied E. The Standard American Diet and its relationship to the health status of Americans.Nutr Clin Pract. 2010;25(6):603-612.
- USDA Economic Research Service. Food Availability (Per Capita) Data System. 2013. http://www.ers.usda.gov/Data/FoodConsumption/FoodAvailIndex.htm.
- Popkin BM, Duffey KJ. Does hunger and satiety drive eating anymore? Increasing eating occasions and decreasing time between eating occasions in the United States. Am J Clin Nutr. 2010;91(5):1342-1347.
- Reedy J, Krebs-Smith S. Dietary Sources of Energy, Solid Fats and Added Sugars among Children and Adolescents in the United States. J Am Diet Assoc. 2010;110(110):1477-1784.
- Pan A, Sun Q, Bernstein AM, et al. Red meat consumption and mortality: results from 2 prospective cohort studies. Arch Intern Med. 2012;172(7):555-563.
- Koeth RA, Wang Z, Levison BS, et al. Intestinal microbiota metabolism of l-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19(5):576-585.
- Micha R, Wallace SK, Mozaffarian D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: a systematic review and meta-analysis.Circulation. 2010;121(21):2271-2283.
- Micha R, Michas G, Mozaffarian D. Unprocessed red and processed meats and risk of coronary artery disease and type 2 diabetes - an updated review of the evidence. Curr Atheroscler Rep. 2012;14(6):515-524.
- Larsson SC, Wolk A. Meat consumption and risk of colorectal cancer: a meta-analysis of prospective studies. Int J Cancer. 2006;119(11):2657-2664.
- Cross AJ, Leitzmann MF, Gail MH, Hollenbeck AR, Schatzkin A, Sinha R. A prospective study of red and processed meat intake in relation to cancer risk. PLoS Med. 2007;4(12):e325.
- Schulze MB, Hu FB. Primary prevention of diabetes: what can be done and how much can be prevented? Annu Rev Public Health. 2005;26:445-467.
- Sinha R, Cross AJ, Graubard BI, Leitzmann MF, Schatzkin A. Meat intake and mortality: a prospective study of over half a million people. Arch Intern Med. 2009;169(6).
- Pollan M. Food Rules: An Eater’s Manual. USA: Penguin Group; 2009.
- Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr. 2006;84(2):274-288.
- Basu S, Yoffe P, Hills N, Lustig RH. The Relationship of Sugar to Population-Level Diabetes Prevalence: An Econometric Analysis of Repeated Cross-Sectional Data. Wagner B, ed. PLoS One. 2013;8(2):e57873.
- Malik VS, Popkin BM, Bray GA, Depres J-P, Willett WC, Hu FB. Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes. Diabetes Care. 2010;33(11):2477-2483.
- Stanhope KL, Bremer A a, Medici V, et al. Consumption of fructose and high fructose corn syrup increase postprandial triglycerides, LDL-cholesterol, and apolipoprotein-B in young men and women. J Clin Endocrinol Metab. 2011;96(10):E1596-E1605.
- Mozaffarian D, Micha R, Wallace S. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PLoS Med. 2010;7:e1000252.
- Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Saturated fatty acids and risk of coronary heart disease: modulation by replacement nutrients. Curr Atheroscler Rep. 2010;12:384-390.
- Laake I, Pedersen JI, Selmer R, et al. A prospective study of intake of trans-fatty acids from ruminant fat, partially hydrogenated vegetable oils, and marine oils and mortality from CVD. Br J Nutr. 2012;108(04):743-754.
- Salmerón J, Hu FB, Manson JE, et al. Dietary fat intake and risk of type 2 diabetes in women. Am J Clin Nutr. 2001;73:1019-1026.
- Hu FB, van Dam RM, Liu S. Diet and risk of Type II diabetes: the role of types of fat and carbohydrate.Diabetologia. 2001;44:805-817.
- Scalbert A, Andres-Lacueva C, Arita M, et al. Databases on Food Phytochemicals and Their Health-Promoting Effects. J Agric Food Chem. 2011;59(9):4331-4348.
- Carkeet C, Grann K, Randolph RK, Venzon DS, Izzy SM, eds. Phytochemicals: Health Promotion and Therapeutic Potential. Boca Raton, FL: CRC Press; 2012.